2022: Volume 4, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFThe Quality of Esthetic Rehabilitation in Undergraduate Level of Gezira University, Sudan
Alfadel Ameer*
BDS, Faculty of Dentistry, University of Gezira, Sudan
*Corresponding author: Alfadel Ameer, BDS, Faculty of Dentistry UOG, University of Gezira, Email: [email protected]
Received Date: November 5, 2022
Publication Date: December 10, 2022
Citation: Ameer A. (2022). The Quality of Esthetic Rehabilitation in Undergraduate Level of Gezira University, Sudan. Dental. 4(1):9.
Copyright: Ameer A. © (2022).
ABSTRACT
Introduction: Full coverage rehabilitation includes extraction of unrestorable severely carious teeth, Scaling and root planning for the teeth including treating gingival, periodontal inflammations and prosthodontics varies from simple restoration, RPD, post and core, and fixed bridges to obtain the desired result that leads to perfect smile design and patient satisfaction in Wad Medani dental teaching hospital, Gezira state Sudan. Case report: In this case, the treatment plan was discussed step by step with the patient in all phases of the treatment to reach the most durable and esthetic result. Conclusion: A thorough history and clinical examination are very important factors in making an accurate diagnosis, which will direct to a treatment plan that will be validated by frequent follow-ups. The patient was delighted with the outcome.
Keywords: smile, esthetic, restoration, scaling and root planning, gingival treatment, periodontal inflammation
INTRODUCTION
Dental rehabilitation: treatment consists of a complete and simultaneous restoration of all the present dental pieces, the replacement of the missing dental pieces of the maxilla and the jaw, and extraction of remaining root and hopeless unrestorable tooth. It helps to establish new aesthetic and functional principles, producing important changes in the person's appearance.
This procedure involves the combination of several treatments such as direct restorations, crowns, bridges, prostheses, and gum surgery. The combination of treatments and areas depends on the dental aesthetic and functional objectives and the patient's demands and needs.
The point of a full mouth reconstruction plan is to optimize the health of the entire mouth, including the teeth, the gums, and the bite.
Patients' demands for aesthetics are growing every day, which is enhancing our everyday work in a smile, however, one of the essential components of a pleasing smile is a healthy periodontium. To achieve the desired aesthetic effect, there must be no periodontal disease symptoms such as pocketing, bleeding, swelling, or irritation. The quantity of gingival display, gingival architecture, clinical crown size, and tooth position, however, all have a significant impact on the cosmetic value of the cosmetic restoration.
Case Report
A 58-year-old female patient with C/O unesthetic appearance & multiple losses of teeth, requiring complete oral rehabilitation to restore the form function and aesthetics. She lost her teeth gradually due to severe caries. First time for the patient to make a denture. She presents with a chief complaint: (I need a new smile). Her expectation was to have the best available treatment regarding her concern in order to eat properly as well as speak clearly (function well)
Intraoral examination reveals healthy normal alveolar mucosa, however, the amount of alveolar bone present is adequate for denture support. The patient is medically fit.
Diagnosis of the chief complaint: Reversible pulpitis in teeth no 11 & 21
Problem list:
- 6 Teeth were extracted (loss of function). Badly decayed maxillary first premolars (Rt & Lt).
- Remaining root of teeth no.23 &36
- Caries on teeth no.26 &34
- Aesthetic concern.
- Short clinical crowns
Periodontal DIAGNOSIS:
- Generalized severe chronic periodontitis.
- Poor oral hygiene.
- Staining and plaque accumulation in lower anterior teeth.
Chart shows:
- PI: 2
- GI: 2
- MO: 0
- PPD: 4
- RE/FI: 3
- PAL: 6
- EOE: Patient looks well, nothing abnormal was detected in eyes and No sign of pain or tenderness in the head and neck area.
- TMJ: no clicking or tenderness in the TMJ area or muscles of mastication.
- IOE: Revealed multiple carious teeth, missing teeth, slight swelling of gingiva, and pigmentation

Image 1: EOE: Patient looks well, nothing abnormal was detected in eyes and No sign of pain or tenderness in the head and neck area. TMJ: no clicking or tenderness in the TMJ area or muscles of mastication. IOE: Revealed multiple carious teeth, missing teeth, slight swelling of the gingiva, and pigmentation.
.png)
Image 2: Patient chart hard tissues identifying the missing and the carious teeth.
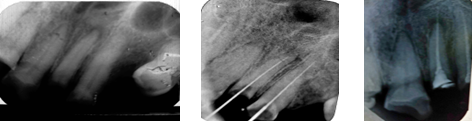
Image 3: Above pictures showing the periapical radiograph of the anteriors, which root canal determination and obturation have been done in order to maintain the vitality of pulp and entomb the remnant bacteria.

Image 4: Gingival retractor cord to obtain ferrule effect & subgingival finish line corresponding to the treatment plan of the fixed partial denture.

Image 5: Lateral incisor is very difficult to preserve due to the periapical granuloma so extraction has been done in this case by bayonet.

Image 6: The upper and lower Removable partial denture ready to be delivered to the patient.


Image 7: Centric occlusion before and after the treatment.

Image 8: Treatment options were discussed with the patient. A decision was made to improve the esthetic appearance of all her upper teeth that show in the smile (including upper second premolars). First, selective crown lengthening would be done to level the gingival margins.
Patient chart hard tissues identifying the missing and carious teeth.
The above pictures show the periapical radiograph of the anteriors, in which root canal determination and obturation have been done in order to maintain the vitality of the pulp and entomb the remnant bacteria.
Gingival retractor cord to obtain ferrule effect & subgingival finish line corresponding to the treatment plan of the fixed partial denture.
The lateral incisor is very difficult to preserve due to the periapical granuloma so extraction has been done in this case by bayonet.
The upper and lower Removable partial denture ready to be delivered to the patient (1-15).
Centric occlusion before and after the treatment
Treatment options were discussed with the patient; it was decided to make all of her visible upper teeth more aesthetically pleasing (including upper second premolars) to level the gingival margins.
Enhancing oral health Instructions for scaling, polishing, and oral hygiene were rigorously followed. After brushing and flossing, chlorhexidine mouthwash 0.2% was recommended twice a day. After one week, a follow-up appointment for periodontal care was given.
The patient was given postoperative instructions and was told to keep using chlorhexidine mouthwash twice daily. After a week, a follow-up appointment was scheduled.
Tooth cleaning and making impressions.
The procedure lasted for four weeks before the prosthetic component was begun.
Saliva ejectors and cotton rolls were used to limit the amount of moisture. There was only one retraction cord employed.
CONCLUSION
In this case study, high-standard quality treatment was an approach for achieving the best possible cosmetic outcome for the maxillary and mandibular teeth. Extraction of unrestorable teeth and retained roots, Periodontal treatment, restoration design, and adhesion, are regarded as crucial elements for clinical success.
With reference to the relevant literature,
Postoperative Instructions
- Brush the appliance daily outside the mouth, with a tapered brush.
- Do not soak partial dentures in solutions containing chlorine bleach.
- Store the clean denture overnight in clean water.
- Never bite it into place (insert and remove by hand).
- Try to speak naturally as well as chew soft foods and hypersalivation is considered normal on the first days.
- Teach the patient how to use COREGA cream when needed.
- If any inquiries or adjustment varieties call me to set an appointment.
REFERENCES
- Kazis H, Kazis AJ. (1960). Complete mouth rehabilitation through fixed partial denture prosthodontics. J Prosthet Dent. 10:296–303.
- Lerner J. (2008). A systematic approach to full mouth reconstruction of the severely worn dentition. Pract Proceed Aesthet Dent. 20:81-87.
- Jones SSM. (1963). The principles of obtaining occlusion in occlusal rehabilitation. J Prosthet Dent. 13:706-713.
- Brecker SC. (1958). Clinical procedures in occlusal rehabilitation. Philadelphia: W. B. Saunders Co, USA.
- Christensen GJ. (2004). Defining oral rehabilitation. J Am Dent Assoc. 135(2):215-217.
- Dawson PE. Functional occlusion from TMJ to smile design. Mosby St. Louis, Elsevier. 2007:18-26, 27-32, 75-83, 429-52.
- Binkley TK, Binkley CJ. (1987). A practical approach to full mouth rehabilitation. J Prosthet Dent 57(3): 261-266.
- Rivera-Moreles WC, Mohl ND. (1992). Restoration of vertical dimension of occlusion in the severely worn dentition. Dent Clin North Am. 36(3):651-664
- Lynch CD, McConnell RJ. (2002). Prosthodontic management of the curve of Spee: use of the Broadrick flag. J Prosthet Dent. 87(6):593-597
- Dawson PE. (1989,) Vertical Dimension. In: Dawson PE. Evaluation, diagnosis and treatment of occlusal problems. Cv Mosby Company, St. Louis Baltimore, Toronto. 56-71.
- Dawson PE. (1989). Anterior Guidance. In: Peter E.Dawson. Evaluation, diagnosis and treatment of occlusal problems. 2nd Ed. Cv Mosby Company, St. Louis Baltimore, Toronto:274-297.
- Lesan G. (2013). A Clinical Report Rehabilitation of Severely Worn Dentition and Partial Edentulism by Fixed and Removable Prostheses. Int J Prosthodontics Restorative Dentistry. 3(2):57-61.
- Neville, BW.; Damn, DD.; Allen, CM.; Bouqout, JE. Pulp and periapical disease. Oral and maxillofacial pathology. 2nd ed. Philadelphia (PA): WB Saunders; 2002.
- Shugars DA, Shugars DC. (2002). Patient Assessment, Examination and Diagnosis, and Treatment Planning. In: Roberson TM, Heymann HO, Swift EJ, editors. Sturdevant's art and science of operative dentistry. 4th ed. USA: Mosby:389-428.
- Carranza FA. Jr. (1999). The Treatment Plan. In: Carranza FA Jr, Newman MG, editors. Clinical Periodontology. 8th ed. Bangalore: Harcourt Asia Pvt. Ltd:399-400.