2019: Volume 1, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFLabial and Mental Foramina of the Mandible: A Cone Beam Computed Tomography Study
Hamdy A Marzook1*, Abeer A El-gendy2, Fawzy RS Darweesh2
1Department of Oral and Maxillofacial Surgery, Mansoura University, Egypt 2Department of Dentistry, Zagazig University, Egypt
*Corresponding Author: Hamdy A Marzook, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Mansoura University, Mansoura, Egypt.
Received: October 28, 2019 Published: November 16, 2019
ABSTRACT
Purpose: Surgical complications in the anterior mandible had been reported. These complications increase the interest into the content and the vascularity of the area. Cone beam computed tomography (CBCT) was used for investigating bony structures. The aim of this study was to evaluate the anatomical features of labial and mental foramina.
Methods: Foramina on the outer surface of the anterior mandible were evaluated in coronal, sagittal, and axial planes of 104 CBCT scans.
Results: Other than mental foramina, 184 foramina were observed in the labial surface of the mandible. The incidence of the labial foramina was 60.58%. Bilateral and unilateral accessory mental foramina were found in 28.85% of cases.
Conclusion: Mandibular labial foramina are frequently seen in CBCT. Wide variations were seen in different neurovascular anatomical landmarks in the anterior mandible including accessory mental foramina. These findings should be considered when planning for anesthesia and surgery in this region.
KEYWORDS: Accessory mental foramen; Anatomical landmarks; Cone beam computed tomography; Labial foramina; Mental foramen
INTRODUCTION
Many complications are associated with surgical interventions in the anterior region of the mandible. Sensory disturbances of the mental nerve after dental implant placement have been reported. Loss of lip sensation may further be complicated by lip biting, impaired speech, and diminished salivary retention, which have a significant impact on patient's lifestyle [1].
Complications associated with symphyseal bone grafts include intraoperative bleeding, wound dehiscence, mental nerve injury, pulp canal obliteration, and a loss of pulp sensitivity in the anterior lower teeth [2,3]. To avoid these complications, total knowledge of the bone anatomy is a must [4]. Before any surgical procedures in the mandibular premolar area, the anatomy of the mental foramen (MF) and canal, as well as the presence of accessory mental foramina (AMF) should carefully be investigated [5].
CBCT is used for diagnostic purposes in oral and maxillofacial surgery and endodontics, particularly for its low cost, easy accessibility and low radiation [6,7]. It was considered to have better accuracy and diagnostic value than periapical films in the detection of interradicular periodontal bone defects [8]. Detailed information was obtained about dentoalveolar structures with CBCT [9]. CBCT is capable of providing sub-millimetre resolution in images with short scanning time [10]. Cone beam computed tomography (CBCT) was used for investigating structures inside bone without dissection. The lingual foramina and canals are from the structures studied by many investigators [11,12].
Many foramina are present on the lingual aspect of the anterior mandible which may have variations in number and position. It is typically visualized as a single round radiolucent canal with a well-defined opaque border [11,13]. Actually, blood vessels and nerves running through these lingual canals often generate anastomosis with neurovascular structures from the mandibular canal and its branches [14]. The median perforating canal (MPC) of the mandible is the canal connecting the median lingual foramen (MLF) and the labial foramen (LaF) [15]. It was previously concluded that the MPC of the mandible, rarely found in humans, is seen in all specimens in Macaca fascicularis because they have no mental protuberance [16]. A high prevalence of these structures was found in many reports [11,12,17,18].
The labial extensions of the lingual foramina and canals were studied by many investigators [17,19]. CT images were used for the identification of the intrabony canals and for the localization of canalicular communications connecting the labial and lingual mandibular plates. These communications mainly appeared as a crossing of the lateral lingual with the incisive canal, but also as an extension of the median lingual canal to the labial plate [19]. MPC was reported in one cadaveric study of the human mandible [15].
The MF as an important mandibular anatomical landmark is located bilaterally. Its location, size, and shape have been studied by many investigators [20-22]. In the current literature AMF, mandibular incisive canal, and buccal foramina (BF) are frequently documented in various species and ancient skulls in addition to living subjects [23-25]. CBCT analysis for labial and buccal mandibular foramina, however, has not been widely evaluated or used in clinical dentistry yet. The term labial foramen is not used up till now for describing foramina on the labial surface of anterior mandible. The term additional foramina is used by some investigators in describing foramina on the labial and lingual surface of anterior mandible [25]. There is a need to establish a well-defined profile for the anatomical characteristics of labial foramina in CBCT. Therefore, the aim of this study was to assess the occurrence and anatomical features of mental, accessory mental and labial foramina and their bony canals in inter foraminal region of the mandible using CBCT.
MATERIAL AND METHODS
Interforaminal segment of the mandible was studied in 104 CBCT scans. Readings from different slices were recorded using Planmeca Romexis Viewer 5.4.1.R. computer program (Planmeca, Italy) for every patient. Of the 104 patients, 73 were female and 31 were male. The average age was 34.86 years. The study protocol was approved by the Ethical Committee of the Faculty of Dentistry, Mansoura University (code 07130818). Scans showing intraosseous lesions or fractures in the target area were excluded. The incidence, location, and types of labial, mental, and accessory mental foramina were evaluated in coronal, sagittal, and axial planes by three investigators. These foramina were assigned into 3 main categories labial, mental and accessory mental foramina. Mental foramina were considered firstly in the left and right sides. Accessory mental foramina were considered only after following the course of their bony canals. Canals intersecting with the inferior alveolar canal in the premolar region are considered either mental or accessory mental canals. Foramina located mesial to canines or their canals contacting incisive nerve mesial to the canine were considerd labial. Recorded foramina were considered only when there is agreement between 2 of the 3 examiners.
RESULTS
A total of 390 foramina on the outer side of the mandible were recorded from coronal, sagittal, and axial planes of 104 CBCT scans. These foramina were assigned into 3 main categories mental, accessory mental, and labial foramina (Table 1). Mental foramina were found to be present in both sides of the mandible in all studied scans (100%). Seventy three patients (70%) showed at least one more foramen other than the bilateral mental foramina.
Table 1: Distribution of foramina along the studied CBCT scans.
|
% |
Bilateral cases |
Number of patients |
Number of readings |
Studied Structure |
No |
|
100% |
104 |
104 |
208 |
Mental foramina |
1 |
|
28.85% |
9 |
30 |
44 |
Accessory mental foramina |
2 |
|
61.54% |
31 |
64 |
58 |
Right Labial foramina |
3 |
|
57 |
Left Labial foramina |
3 |
|||
|
11 |
Symphyseal Labial foramina |
3 |
|||
|
12 |
Submental Labial foramina |
4 |
|||
|
4.8% |
0 |
5 |
5 |
Alveolar or interseptal Labial foramina |
5 |
Accessory mental foramina were found to be present in 30 patients (28.85%), 21 females and 9 males. Their total number was 44 foramina. Different locations of accessory mental foramina in relation to mental foramina were found. More than one accessory mental foramen was recorded in 11 patients either unilaterally or bilaterally. Accessory mental foramina were found to be smaller than mental foramina (Figure 1). Variations in size of accessory mental foramina and location in relation to mental foramina could be seen in many cases. Nine cases showed bilateral accessory mental foramina and those were seen in coronal (Figure 2), axial (Figure 3), and sagittal planes according to their locations.
Figure 1: An axial plane section showing a large mental foramen (MF) in the right side and smaller mental foramen and accessory mental foramen (AMF) in the left side.
Figure 2: A coronal section showing bilateral inferior accessory mental foramina (AMF).

Figure 3: Axial plane section showing bilateral accessory mental foramina (AMF) with wide horizontal area with mental foramina (MF).
Labial foramina were recorded in 64 (61.54%) patients. Their total number was 138 foramina. More than one labial foramen was recorded in 38 patients (Table 2). Labial foramina could be seen in 3D images mimicking AMF. These could be also seen in different planes: coronal, sagittal, and axial planes (Figure 4). Different locations of labial foramina: symphyseal or midline, lateral, alveolar or interseptal, and sub mental were recorded (Figure 5). Evidence of connection between lingual and labial foramina could be proved in many cases (Figure 6). Abnormal variations of mandibular foramina such as bony condensation related to foraminal canal, descending canal from a labial foramen, and large size mental foramina were also seen.
Table 2: Distribution of labial foramina along the studied CBCT scans.
|
% of total 104 cases |
Total foramina |
Number of patients |
Number of foramina |
|
25% |
26 |
26 |
1 |
|
19.23% |
40 |
20 |
2 |
|
8.65% |
27 |
9 |
3 |
|
4.81% |
20 |
5 |
4 |
|
1.92% |
10 |
2 |
5 |
|
0% |
0 |
0 |
6 |
|
0.96% |
7 |
1 |
7 |
|
0.96% |
8 |
1 |
8 |
|
61.5% |
138 foramina |
64 patients |
Total |
Figure 4: Appearance of the labial foramen (LaF) in different views: a) coronal, b) sagittal, and c) axial images.

Figure 5: Different locations of labial foramina: a) symphyseal or midline, b) lateral, c) alveolar or interseptal, and d) sub mental.
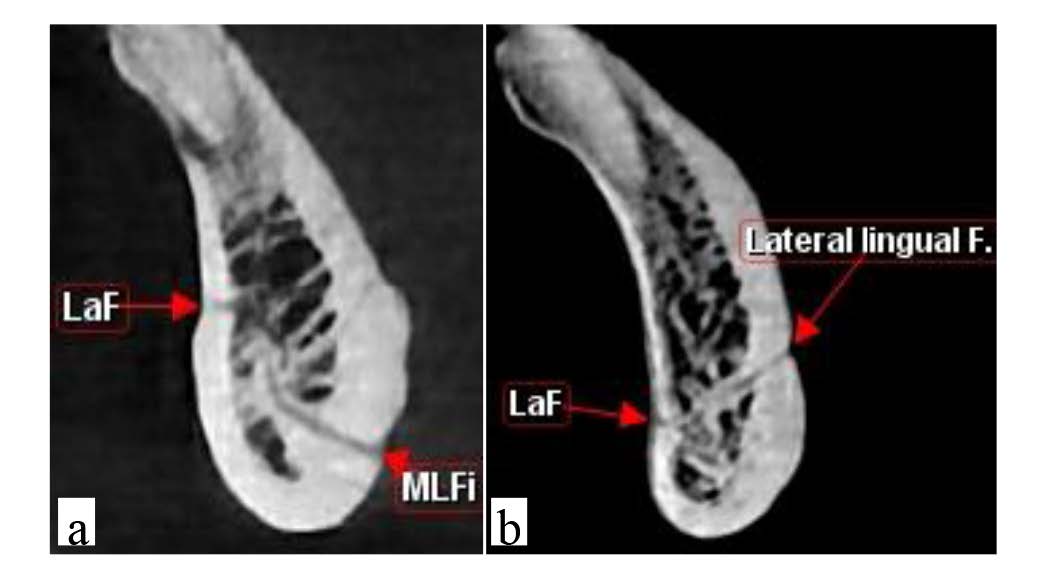 Figure 6: Different communications of labial foramina (LaF) with a) median lingual foramen (MLFi) and b) lateral lingual foramen.
Figure 6: Different communications of labial foramina (LaF) with a) median lingual foramen (MLFi) and b) lateral lingual foramen.
DISCUSSION
Complications related to surgical interventions in the anterior segment of the mandible had been reported such as unexplained bleeding and sensory disturbances [26,27]. These complications increases the interest into the content and the vascularity of the area [28-30]. To avoid intraoperative and postoperative hemorrhage, neurosensory loss, the locations of neurovascular structures must be identified before implant placement, genioplasty, chin graft, or endodontic surgery in the anterior mandible. Osseous neurovascular structures include the MF, the AMF, and LaF or buccal foramina [31-33].
In this study, identified defects of the buccal cortical plate were classified as MF, AMF and LaF. At least one MF was found in both sides in all the studied scans (100%). These results are in agreement with many previous studies [5,34,35]. We considered AMF as a foramen connecting with mandibular canal and smaller than MF. In our sample of Egyptian cases, there was a relatively high incidence of AMF. This result is in accordance with the conclusion of Hanihara, et al. [36] that it is most common in Central Asians and Subsaharan Africans among recent human populations.
There was a prevalence of the labial foramina than accessory mental foramina for all CBCT images, with significant variations of their locations and anatomical characteristics. Nutrient foramina in the buccal cortical plate were found by Naitoh, et al. [24] to be much more common than AMFs. Labial foramina could be detected in different locations. Symphyseal, lateral symphyseal, sub mental and canine region foramina could be observed. In most instances labial foraminal canals were found in the lower half of mandibular height and were directed to the middle of the mandible and lingually. To the best of our knowledge studies investigating the location and orientation of labial foraminal canals are rare. Additional foramina was the term used by Kabak, et al. [25] to describe a group of foramina other than mental and AMF which were located on the buccal and/or lingual surfaces of the mandibular body.
Labial foraminal canals were found to be connected to incisive canal or lingual foramina in many cases. Median perforating canal was recorded in 28 cases (26.92%). This result support the findings of a previous report of a rare case of an artery passing through the median perforating canal of the mandible [15]. More than one median perforating canal was detected in two cases. There is no other conclusive evidence in the literatures that more than one canal is present in humans.
Many of the lingual and labial canals were connected indirectly through contacting the incisive canal. These results are inaccordance with that of Trikeriotis et al. [19] whose results showed anastomosis between lingual canals with the incisive canal and presence of a network or a plexus of canals in the anterior region of the mandible.
In our study five cases showed higher positions of LaF. Of course, possibility of nutrient canals which was postulated by many researchers should be considered [17-19]. Evidence-based studies do not clearly show this.
In this study, the labial foramina showed high incidence than previously considered for them. It is not safe to recommend any bone graft or implant surgery in the anterior region of the mandible without CBCT study of the region. In our Egyptian sample, there was a significant variability in the mandibular LaF and their bony canals anatomy and location. This was in agreement with the finding of other studies [16,17,19]. Knowledge of the anatomical variations of neurovascular canals is necessary to preserve these structures during surgical procedures of mandible and preventing complications. To the best of our knowledge, this study was the first to investigate the radiographic anatomy of labial foramina of the anterior mandible in Egyptian population.
CONCLUSION
The results of this study showed that mandibular labial foramina and bony canals are frequently present in mandibles with wide variations in CBCT. In the lateral to symphysis, the incidence of foramina was the highest in this region. The prevalence of accessory mental foramina in Egyptian population is relatively high. These findings should be considered in diagnosis and planning for anesthesia and surgery in the lower anterior region to prevent possible complications. A preoperative thorough investigation of the symphyseal and parasymphyseal regions using CBCT is highly recommended when targeting surgical interventions in these areas.
Acknowledgments
The authors would like to acknowledge Myray dental radiology center for suppling the dicom files. The authors have no conflict of interest to declare.
Author Contribution
HA Marzook: Project development, Data Collection, Manuscript writing
AA Elgendy: Data collection, Data analysis, Manuscript revising, Final approval
FA Darweesh: Data collection, Data analysis, Manuscript revising, Final approval
Conflict of Interest
Funding: This study was funded by X (grant number X).
Conflict of Interest: Author A has received research grants from Company A. Author B has received a speaker honorarium from Company X and owns stock in Company Y. Author C is a member of committee Z.
REFERENCES
- Wismeijer D, van Waas MA, Vermeeren JI, Kalk W (1997) Patients perception of sensory disturbances of the mental nerve before and aftewr implant surgery. A prospective study of 110 patients. Br J Oral Maxillofac Surg 35: 254-9.
- Noia CF, Ortega-Lopes R, Olate S, Duque TM, de Moraes M and Mazzonetto R (2011) Prospective clinical assessment of morbidity after chin bone harvest. J Craniofac Surg 22(6): 2195-2198.
- Raghoebar GM, Louwerse C, Kalk WW, Vissink A (2001) Morbidity of chin bone harvesting. Clin Oral Implants Res 12(5):503-507.
- Greenstein G, Cavalklaro J, Romanos G, Tarnow D (2008) Clinical recommendations for avoiding and managing surgical complications associated with implant dentistry. A review. J Periodontol 79(8): 1317-1329.
- Babiuc I, Pauna M, Matelas C, Tanase G, Mihal A (2017) CBCT study on the anatomy of the mental foramen and canal in Romanian population. Acta Medica Transilvanica 22(3): 61-63.
- De Vos W, Casselman J, Swennen GRJ (2009) Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: A systematic review of the literature. Int J Oral Maxillofacial Surg 38(6): 609-625.
- Iikubo M, Kobayashi K, Mishima A, Shimoda S, Daimaruya T (2009) Accuracy of intraoral radiography, multidetector helical CT, and limited cone-beam CT for the detection of horizontal tooth root fracture. Oral Surg Oral Med Oral pathol Oral Radiol Endod 108(5): e70-74.
- Noujeim M, Prihoda TJ, Langlais R, Nummikoski P (2009) Evaluation of high-resolution cone beam computed tomography in the detection of simulated interradicular bone lesions. Dentomaxillofacial adiol 38: 156-162.
- Ilguy D, Ilguy M, Fisekcioglu E, Bayirli G (2009) Detection of jaw and root fractures using cone beam computed tomography: A case report. Dentomaxillofacial Radiol 38(3): 169-173.
- Scarfe WC, Farman AG, Sukovic P (2006) Clinical applications of cone-beam computed tomography in dental practice. JCDA 72(1): 75-80.
- Denny CE, Natarajan S, Ahmed J, Binnal A, Jindal R (2016) Anatomic variation in lingual foramen: A cone beam computed tomography study. World J Dent 7(4): 179-81.
- Wang YM, Ju YR, Pan WL, Chan CP (2015) Evaluation of location and dimensions of mandibular lingual canals: A cone beam computed tomography study. Int J Oral Maxillofacial Surg 44(9): 1197-1203.
- Sheikhi M, Mosavat F, Ahmadi A (2012) Assessing the anatomical variations of lingual foramen and its bony canals with CBCT taken from 102 patients in Isfahan. Dent Res J 9(Suppl 1): S45-51.
- Arx von T, Lozanoff S (2016) Lingual foramina and canals. Clin Oral Anat 463-487.
- Iwanga J, Watanabe K, Saga T, Tabira Y, Yamaki K (2016) A rare case of an artery passing through the median perforating canal of the mandible. Case Rep Dent 8183565.
- Iwanga J, Watanabe K, Saga T, Tabira Y, Hirasaki E (2017) Radiological and microsurgical anatomy of the mandible: Comparative study of human and Macaca Fascicularis. Anat Record 300(8): 1464-1471.
- Babiuc I, Tarlungeanu I, Pauna M (2011) Cone beam computed tomography observations of the lingual foramina and their bony canals in the median region of the mandible. Rom J Morphol Embryol 52(3): 827-829.
- Locks BJC, Claudins M, Azevedo-Alanis LR, Ditzel AS, Fontao FNGK (2018) Evaluation of the bone anatomy of the anterior region of the mandible using cone beam computed tomography. Rev Odontol UNESP 47(2): 69-73.
- Trikeriotis D, Paravalou E, Diamantapoulos P, Nikalaou D (2008) Anterior mandible canal communications: A potential portal of entry for tumour spread. Dentomaxillofac Radiol 37(3): 125-129.
- Singh R, Srivastav A (2010) Study of position, shape, and size and incidence of mental foramen and accessory mental foramen in Indian adult human skulls. Int J Morphol 28(4): 1141-1146.
- Leite GM, Lana JP, de Carvalho Machado V, Manzi FR, Souza PE (2014) Anatomic variation and lesions of the mandibular canal detected by cone beam computed tomography. Surg Radiol Anat 36(8): 795-804.
- Khojastepour L, Mirbeigi S, Mirhadi S, Safaee A (2015) Location of mental foramen in a selected Iranian population. A CBCT assessment. Iran Endod J 10(2): 117-121.
- Naitoh M, Hiraiwa Y, Aimiya H, Gotoh K, Ariji E (2009a) Accessory mental foramen assessment using cone-beam computed tomography. Oral Surg Oral Med Oral pathol Oral Radiol Endod 107(2): 289-294.
- Naitoh M, Nakahara K, Hiraiwa Y, Aimiya H, Gotoh K (2009b) Observation of buccal foramen in mandibular body using cone-beam computed tomography. Okajiamas Folia Anat Jpn 86(1): 25-29.
- Kabak SL, Savrasova NA, Melnichenko YM, Zhuravleva NV (2017) Imaging of accessory buccal foramina using cone-beam computed tomography: Case reports. Eur J Anat 21(3): 189-195.
- Isaacson TJ (2004) Sublingual hematoma formaton during immediate placement of mandibular endosseous implants. J Am Dent Assoc 135(2): 168-172.
- Deng W, Chen SL, Huang DY (2009) Traumatic neuroma of mental nerve following chin augmentation. Int J Oral Maxillofac Surg 38(12): 1324-1326.
- Liang X, Jacobs R, Corpas LS (2009) Chronologic and geographic variability of neurovascular structures in the human mandible. Forensic Sci Int 190(1-3): 24-32.
- Tirumala Ravali C (2017) Prevalance of mandibular incisive canal in CBCT: A retrospective study. Int J Applied Dental Sci 3(4): e238-240.
- Assari A, Almashat H, Alamry A, Algarni B (2017) Prevalence and locaton of the anterior lingual foramen: A cone-beam computed tomography assessment. Saudi J Oral Sci 4(1): 41-45.
- Babbush CA, Hahn JA, Krauser JT, Rosenlicht JL (2010) Dental implants: The art and science. W. B. Saunders, Philadelphia, USA, P. 544.
- Tagaya A, Matsuda Y, Nakajima K, Seki K, Okano T (2009) Assessment of the blood supply to the lingual surface of the mandible for reduction of bleeding during implant surgery. Clin Oral Implants Res 20(4): 351-355.
- Rosano G, Taschieri S, Gaudy JF, Testori T, Del Fabbro M (2009) Anatomic assessment of the anterior mandible and relative hemorrhage risk in implant dentistry: A cadaveric study. Clin Oral Implants Res 20(8): 791-795.
- Mbajiorgu EF, Mawera G, Asala SA, Zivanovic S (1998) Position of the mental foramen in adult black Zimbabwean mandibles: A clinical anatomical study. Cent Afr J Med 44(2): 24-30.
- Chono BS, Gohil K, Powar R, Makdissi J (2017) Anatomical relationship between mental foramen, mandibular teeth and risk of nerve injury with endodontic treatment. Clin Oral Investig 21(1): 381-387.
- Hanihara T, Ishida N (2001) Frequency variations of discrete cranial traits in major human populations. IV. Vessel and nerve related variations. J Anat 199(pt 3): 273-287.
Copyright: Marzook HA, et al. © 2019. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Marzook HA (2019). Labial and Mental Foramina of the Mandibe: A Cone Beam Computed Tomography Study. Dental 1(1): 1.